After the hurricane Maria hit, Puerto Rico experienced unprecedented disruption of the medical infrastructure: in the first 3 days following the hurricane, only 3 major hospitals were functioning and even 2 weeks later only 25 of the commonwealth’s 68 hospitals were operational. Prescription drugs shortage and limited access to medical care quickly provoked aggravation of common chronic diseases such as asthma, cardiovascular disease, chronic renal disease, diabetes, and HIV. As the disaster response did not reach the rural areas for weeks after the hurricane, people there were especially affected by exacerbations of these illnesses. [1]
“Although the initial mortality estimates following the storm were low, more recent estimates have placed the death toll in the thousands, after including indirect deaths resulting from worsening of chronic conditions or from delayed medical treatments.” — Community Pharmacy Response in the Aftermath of Natural Disasters, 2018 [1]
Unable to receive their usual medical aid, countless patients reached out to their community pharmacists as to the first health care providers available.
“The role of community pharmacists following a natural disaster has previously been documented, and may include the triage of evacuees, assessment of immunization needs, and provision of prescription medications under a collaborative practice agreement. However, our experience in Puerto Rico demonstrated a variety of barriers that limited pharmacists’ ability to adequately respond to the magnitude of this disaster.” — Community Pharmacy Response in the Aftermath of Natural Disasters, 2018 [1]
The mentioned barriers included power outage, disrupted communication, and medication shortage due to nonexistent or severely limited distribution. [1]
To effectively help the community after disasters, selected pharmacies should be specially equipped and prepared. To ensure this, in times of anticipated crisis we recommend two preemptive major steps: research PR’s medical needs and ensure access to electronic medical records (EMR), means of communication, and drugs refrigeration during an emergency.
Research of Puerto Rico’s Medical Needs
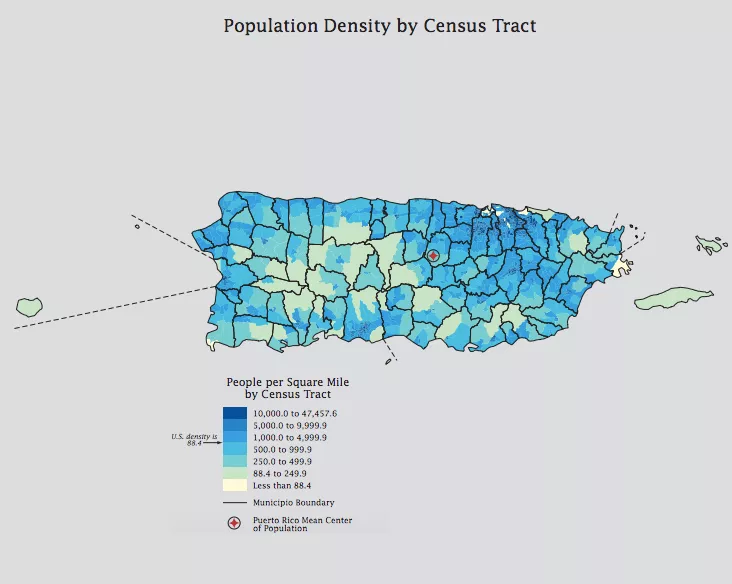
As mentioned in the article “Community Pharmacy Response in the Aftermath of Natural Disasters,” [1] the limited data that exists from the continental United States may not be truly representative of Puerto Rico’s unique geographic and sociopolitical context. Thus, more information should be gathered in order to evaluate the need of heat-sensitive medications (insulin, vaccines to infectious diseases etc.) and medications to chronic diseases (asthma, cardiovascular diseases, diabetes etc.). Such statistics are usually gathered by the Puerto Rico Department of Health and should include:
- Determining and prioritizing the most widespread conditions and diseases.
- Determining the number of people in need of treatment.
- Determining the amount of medication needed per capita for specific time periods (aiming at redundancy).
Survey methods for health data collection include [4]:
- Personal interviews in households and via phone.
- Standardized physical examinations, diagnostic procedures, dental examinations, and laboratory tests in mobile examination centers.
- Review of facility information and patient medical records in hospitals, hospital emergency and outpatient departments, physicians’ offices, nursing homes, home and hospice care agencies, and residential care facilities.
Access to EMR, Means of Communication, and Drugs Refrigeration During an Emergency
As the article “Community Pharmacy Response in the Aftermath of Natural Disasters” [1] states, after Maria “countless patients lacked not only their maintenance medications but also any record of what medications of which they were in need.” The main solution to such a problem is the use of EMR.
“The events surrounding Superstorm Sandy in 2012 made it apparent that, with relatively little additional effort and investment, health care providers with EHR [electronic health records] systems may be able to use those systems for patient care purposes even during disasters that result in damage to buildings and facilities, widespread power outages, or both.” — Electronic Health Records Access During a Disaster, 2014 [2]
The EMR penetration rate for Puerto Rico is 85% [3], so the main task is to provide power sources to make EMR accessible during emergencies.

Meanwhile, pharmacists could advise patients to [5]:
- Keep a current list of medications on hand, including dosage and indication.
- Keep a log of how much medication they have.
- Receive early refills in the event of limited pharmacy access. (Thorough guidelines [11] for avoiding inappropriate use of drugs were posted for pharmacists by Arizona Prescription Drug Misuse and Abuse Initiative).
- Place medication in water-tight containers to prevent exposure to floodwater.
- Have ice handy for refrigerated medications (dry ice is a good option).
It might be useful to hand out brochures with these precautions to pharmacy customers.
Aside from the physical access to electronic resources, emergency power sources are needed for storing heat-sensitive medications and сharging communication devices to make contacting prescribers, disaster relief agencies, and third-party payers possible. However, there is another communication necessity – internet and cellular connection (see ‘Cellular service’ section). Although the choice of generator type and direct calculation of their costs requires particular knowledge of statistical data on community needs and internal organization of pharmacies, the following steps for determining necessary information might be of interest:
- Research PR community’s needs.
- Based on this research, determine the number of pharmacies for each municipality that need to be equipped with emergency generators to ensure the availability of necessary medication for all local patients.
- Determine the number of storage refrigerators and computers needed in each of said pharmacies.
- Taking into account the technical characteristics of said refrigerators and computers and the availability of fuel or applicability of renewable sources of energy, choose the type and number of generators needed for each pharmacy.
- Calculate the cost.
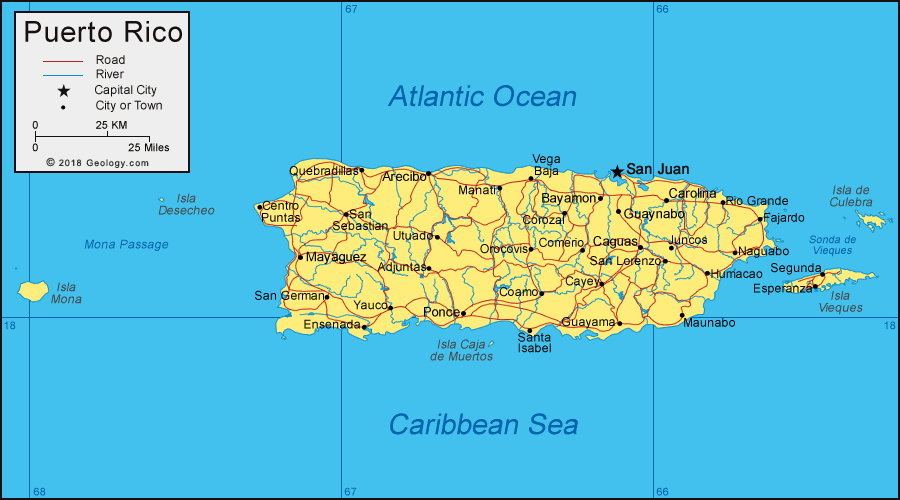
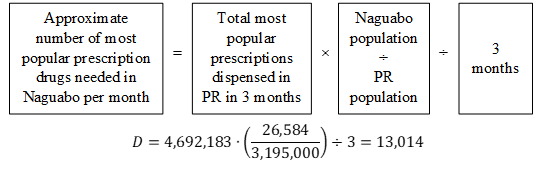
To provide an approximated example of the calculation, we chose the municipality of Naguabo as a case study. We replaiced the required comprehensive research information by the general data about the number of pharmacists available in the US and 200 most popular prescriptions dispensed in Puerto Rico just before hurricane Maria hit.
- 3,195,000 – Puerto Rico population (2018, United States Census Bereau).
- 26,584 – Naguabo population (2017) [12].
- 4,692,183 – number of top 200 prescription drugs dispensed in Puerto Rico during June–August, 2017 (they account for approximately 80% of all prescription drugs dispensed then) [7].
- 18 out of top 200 prescriptions should be refrigerated [9].
- Assume that the average heat-sensitive prescription needs 100 ml of space.
- Assume that a typical refrigerator has volume of 600,000 ml and power of 320 W.[10]
- There are 10.515 pharmacists per 10,000 people in the US (2015) [8].
- Assume that a typical pharmacy laptop has power of 50 W.
- Assume that a typical pharmacy is open for 12 hours each day.
- A unit of the solar powered generator KaliPAK suggested in the ‘Energy’ section of this Proposal has capacity 558 W⋅h and currently costs $365.55.

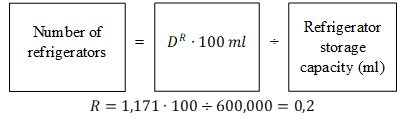
Thus, according to such an approximate calculation, 1 refrigerator should be enough for 1-month stock of necessary heat-sensitive medication. So, refrigeration will need 320 W.
Assuming that the necessary number of computers (C) is the same as the number of pharmacists (P):
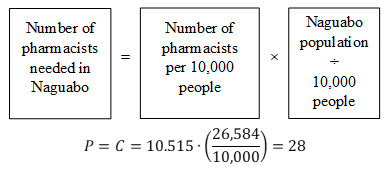
So, the laptops will need 28×50=1,400 W. All in all, generators should provide 1,720 W of power or 1,720×12 (hours) =20,640 W⋅h of energy per day. To provide it, 20,640÷558=37 KaliPAK units are needed. They cost 37×$365.55=$13,525.
Actual calculation should take into account:
- Region-specific statistics on diseases and most needed drugs (not available).
- Region-specific number of pharmacists needed to effectively assist customers.
- The impact of the number of pharmacies on the number of refrigerators. All the pharmacists cannot work at the same facility; thus, they will need more than one refrigerator to avoid the transportation of drugs from one pharmacy to another.
- Facility-specific information about the preferred refrigerator types and the amount of space needed for heat-sensitive prescriptions.
- The actual ratio between the number of pharmacies and the number of computers needed.
- The energy needed for air conditioners (to keep the required temperature in the storage rooms) and phone chargers.
- The choice of the most efficient type of generator and its wholesale price (which is lower than a unit price).
- Other factors connected with power grid instability etc.
The following are on the list of actions to eventually complete, but have been prioritized against so we could focus more on emergency power sources:
- Create emergency protocols for pharmacists. The protocols may be based on a comprehensive set of guidelines [6] suggested by the International Pharmaceutical Federation (FIP).
- Provide extra mental healthcare resources: focus on training staff in Community centers (see ‘Community centers’ section) and spread information about the services such as the Disaster Distress Helpline.
- Using GIS-based methods, propose new pharmacy locations and reinforcement to ensure their geographical accessibility and the adequate ratio between their number and local population.
- Improve storage condition in Community Pharmacies and replace inactivated vaccines.
- ‘Speed up’ the lift of government limitations (e.g. Jones Act).
Some clarifications:
- Triage is the sorting of people according to the urgency of their needs.
- Collaborative practice agreements are used to create formal relationships between pharmacists and physicians or other providers that allow for expanded services the pharmacist can provide to patients and the healthcare team.
- Penetration rate is the percentage of healthcare institutions that use EMR.
- Dispensing is filling or refilling drug containers with prescription drugs for subsequent use by a patient.
- The Substance Abuse and Mental Health Services Administration’s Disaster Distress Helpline provides crisis counseling (24 hours a day, 365 days a year) for those experiencing emotional distress due to natural or human-made disasters. This service is provided in more than 100 languages and is confidential [13].
- The Jones Act requires goods shipped between U.S. ports to be transported on ships that are built, owned, and operated by United States citizens or permanent residents. For Puerto Rico, it inflates shipping costs and increases the time of recovery.